Introduction
Endobronchial lesions refer to abnormalities, benign or malignant, that originate from the bronchial wall. These lesions can vary in their histopathological nature, encompassing conditions such as squamous cell carcinoma, adenocarcinoma, small cell carcinoma, and rare benign tumors like lipomas. The clinical presentation of endobronchial lesions is often non-specific, with symptoms like chronic cough, hemoptysis, chest pain, and shortness of breath, making it difficult to distinguish between benign and malignant lesions based on clinical signs alone.1, 2
Radiologically, endobronchial lesions can manifest as masses, atelectasis, or obstructive pneumonia, but their appearance may overlap significantly with other pulmonary diseases, including infections like tuberculosis. This overlap, especially in countries with a high prevalence of tuberculosis, often leads to diagnostic challenges, as patients may initially receive empiric anti-tuberculosis treatment (ATT), delaying the diagnosis of malignancies.
Fiberoptic bronchoscopy has emerged as a crucial diagnostic tool for evaluating endobronchial lesions. It allows for direct visualization of the bronchial tree, identification of abnormalities, and biopsy for histopathological examination. Unlike other diagnostic modalities like computed tomography (CT) or ultrasound-guided biopsies, bronchoscopy is minimally invasive and provides a higher yield in diagnosing centrally located lesions, especially those associated with lung cancer.2, 3
Lung cancer remains the most common cause of cancer-related deaths worldwide,4 and early diagnosis is essential for improving patient outcomes. Squamous cell carcinoma, strongly linked to smoking, tends to occur centrally in the lungs, while adenocarcinoma, more prevalent in non-smokers and females, often arises in the peripheral lung areas.2 However, both can present as endobronchial lesions, and their early detection through bronchoscopy can significantly impact treatment decisions and survival rates.
This study aims to assess the clinical, radiological, and histopathological characteristics of patients with endobronchial lesions diagnosed through fiberoptic bronchoscopy. By understanding the profiles of these patients, we also hope to highlight the importance of Fiberoptic bronchoscopy in diagnosing these conditions and reducing diagnostic delays.
Materials and Methods
Study design
This is a retrospective study conducted at the Department of Respiratory Medicine, BMC&H, Chitradurga, between March 2020 and July 2023. The study included patients who were diagnosed with endobronchial lesions using Fiberoptic bronchoscopy. Ethical approval for the study was obtained from the institutional ethical committee.
Study population
A total of 180 patients underwent flexible video-bronchoscopy during the study period. Endobronchial lesions were detected in 32 patients, out of which 3 had inconclusive histo-pathological reports and therefore excluded from the study. As a result, 29 patients were included in the study.
Data collection
Data were collected from medical records, including demographic information (age, gender), smoking history, clinical symptoms, radiological findings, and bronchoscopy results. Histopathological reports from the biopsy samples obtained during bronchoscopy were reviewed to classify the lesions into different categories such as squamous cell carcinoma, adenocarcinoma, small cell carcinoma, and benign tumors.
Statistical analysis
Descriptive statistics were used to summarize the demographic, clinical, radiological, and histopathological characteristics of the patients. The results were presented as frequencies and percentages for categorical variables such as gender, smoking status, and histopathological findings.
Results
Age and gender distribution
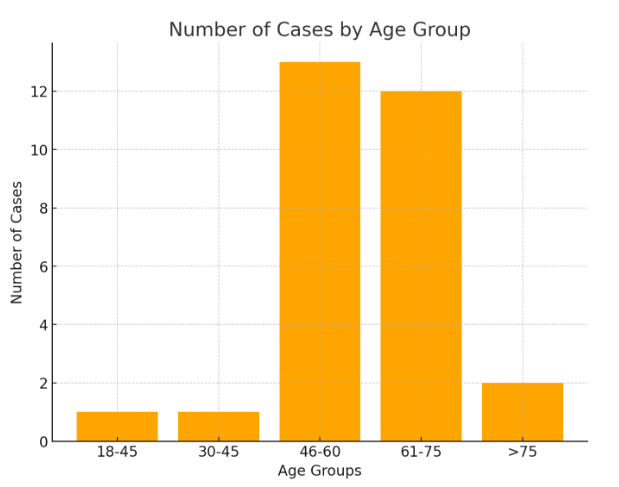
The study involved 29 patients with endobronchial lesions diagnosed via fiberoptic bronchoscopy. The age distribution of patients ranged widely, with most cases (n=13) falling in the middle-aged and elderly groups (Figure 1). Males were predominantly affected, accounting for 65.51% of cases (n = 19), while females comprised 34.48% (n = 10). This gender disparity reflects the higher incidence of smoking in males, which is a significant risk factor for lung cancer and related malignancies.
Smoking history
A significant finding of the study was the high prevalence of smoking among the patients. Of the 29 cases, 16 (55.17%) were smokers, whereas 13 (44.82%) were non-smokers.
Clinical presentation
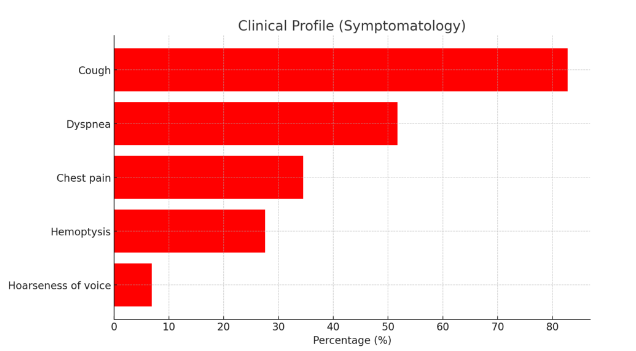
The clinical profile of patients shows a variety of symptoms, with cough being the most prevalent, observed in 82.75% of cases. This is followed by dyspnea, reported by 51.72% of patients. Chest pain was noted in 34.48% of cases, while hemoptysis was present in 27.58% of patients. Hoarseness of voice was the least common symptom, affecting only 6.89% of cases (Figure 2).
Radiological findings, site of involvement and type of lesion
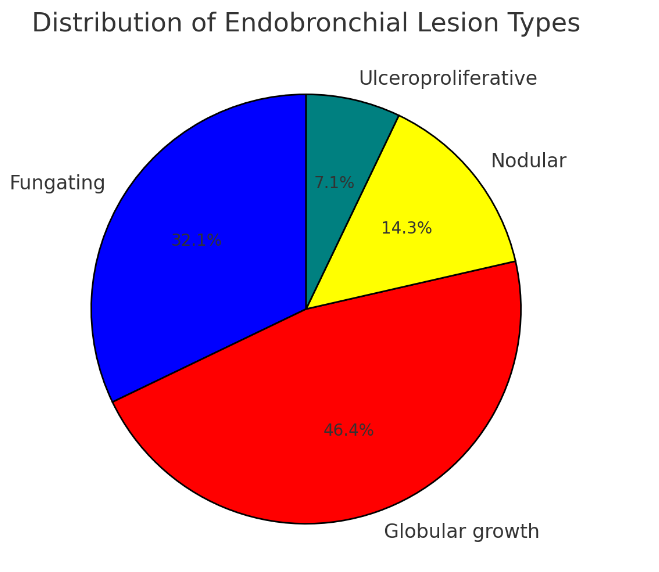
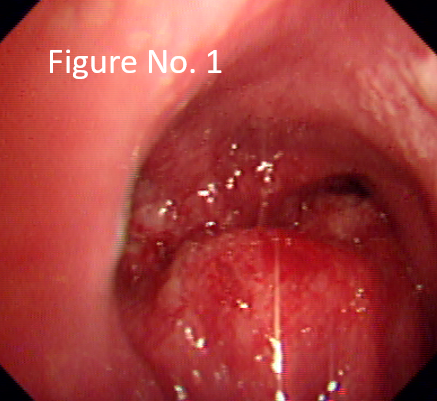
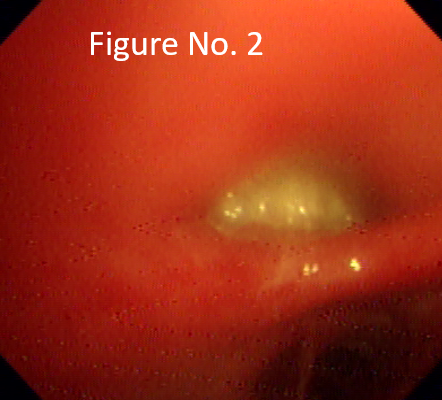
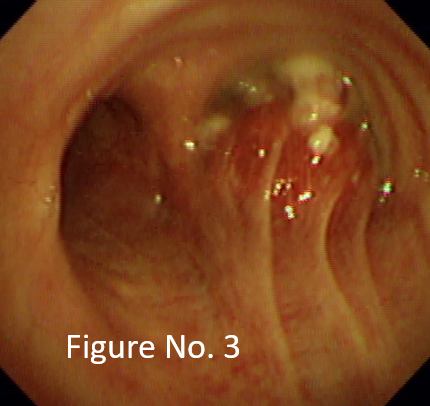
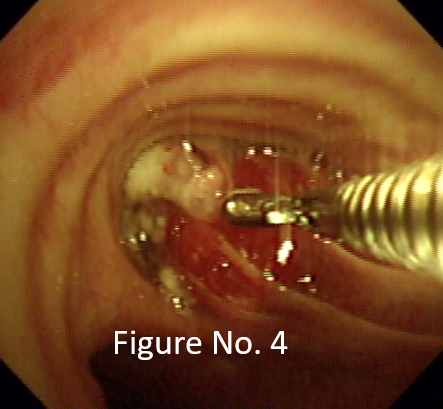
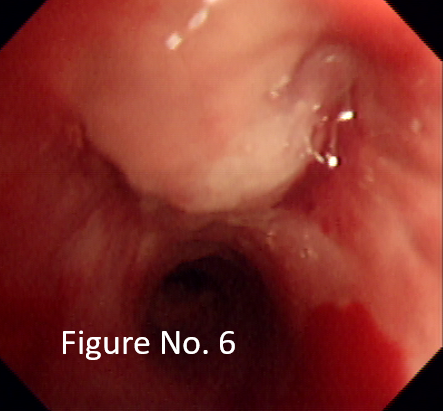
Radiologically, most of the lesions presented as masses (62.06%) (Table 1). The right main bronchus was the most common site of lesion involvement (31.03%) (Table 2). Most of the endobronchial lesions were globular type (46.4%) (Figure 4 ) (Figure 3). Table 1 summarizes Contrast-Enhanced Computed Tomography (CECT) findings among the patients studied. Table 2 Summarizes the site of lesions involved among patients studied.
Table 1
Contrast-enhanced computed tomography (CECT) findings
|
CECT finding |
Number of cases |
Percentage (%) |
|
Cavitary |
5 |
17.24 |
|
Mass/Consolidation |
18 |
62.06 |
|
Mediastinal Lymphadenopathy |
3 |
10.34 |
|
Effusion |
3 |
10.34 |
Table 2
Site of lesions involved among patients studied
|
Site of lesion |
Number of cases |
Percentage (%) |
|
Right main bronchus |
12 |
41.37 |
|
Left main bronchus |
8 |
27.58 |
|
Trachea |
4 |
13.79 |
|
Right upper lobe bronchus |
3 |
10.34 |
|
Left upper lobe bronchus |
2 |
6.89 |
|
Total |
29 |
100 |
Graph 3
Highlights different types of endobronchial lesions visualized on bronchoscopy among patients studied
Histopathological findings
The histopathological distribution of endobronchial lesions reveals a predominance of squamous cell carcinoma and adenocarcinoma among the cases studied. Squamous cell carcinoma was the most common type, accounting for 12 cases (42.85%), followed closely by adenocarcinoma with 10 cases (34.48%). Small cell carcinoma was observed in 5 cases (17.24%), representing a significant proportion but less common than the two leading types. Less frequent lesions included endobronchial lipoma and small round cell tumor, each recorded in only 1 case (3.48%) (Figure 10).
Graph 4
Summarize the distribution of different histopathological findings among the patients studied.
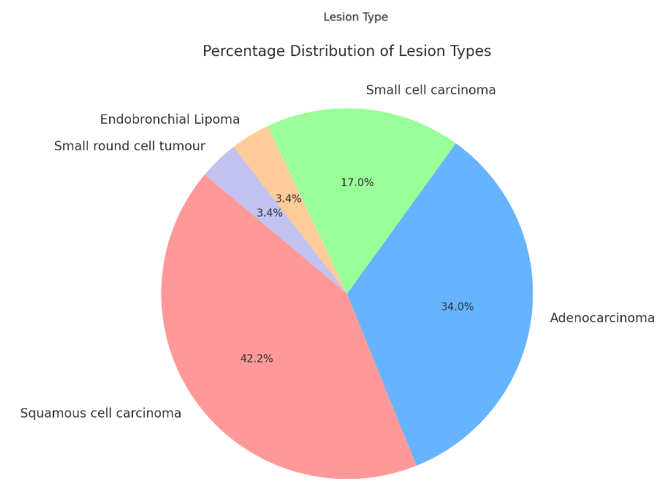
Table 3
Summarizes the biopsy findings, including the number of cases per lesion type and their distribution by smoking status and gender
Discussion
The age distribution of patients ranged widely, with most cases falling in the middle-aged and elderly groups which highlights the fact that risk of lung carcinoma increases with age.1 Males were predominantly affected, accounting for 65.51% of cases (n = 19), while females comprised 34.48% (n = 10). This gender disparity reflects the higher incidence of smoking in males, which is a significant risk factor for lung cancer and related malignancies.1, 5 Cough was the most common symptom which was present in 82.75% of cases, quite similar to previous published studies such as Rana et al.5 Sharma et al., 6 and Khaled et al.7
Radiologically, 62.06% of the lesions presented as masses. This finding was similar to other case studies. 6, 7, 8, 9 Most common endobronchial lesions was an exophytic lesion with globular type accounting for 46.4% of the cases. Similar findings were reported in study by Sharma et al (2022) and Rabahi et al., 1, 10 Additionally, most lesions commonly involved the right main bronchus accounting for 41.37% of the cases.
Squamous cell carcinoma was the most common type of malignancy, accounting for 42.85% of cases. The high percentage of smokers underscores the well-documented association between tobacco use and the development of endobronchial malignancies. 2 The strong association between smoking and squamous cell carcinoma was evident in this study, as 55.17% of the patients had a smoking history. This is consistent with existing literature that links squamous cell carcinoma to central airway involvement and its predilection for smokers. According to Chhajed et al. (2002), squamous cell carcinoma often presents with symptoms such as cough and hemoptysis due to the tumor's central location in the bronchi. 2 In contrast, Adenocarcinoma, which constituted 34.48% of cases, typically arises peripherally and is more common in non-smokers and females, which was reflected in the study results. The relatively lower number of benign lesions, such as lipomas, reflects their lesser occurrence but significant clinical relevance when detected. According to Brambilla et al. (2001), adenocarcinoma now represents the most common histological subtype of lung cancer in non-smokers.11 The high incidence of malignancy in the study, especially squamous cell carcinoma and adenocarcinoma, is consistent with global trends in lung cancer epidemiology, where these are among the most common histological types.
Other benign lesions like endobronchial tuberculosis, aspergillosis was not detected in our study. Although these lesions constitute a small proportion of endobronchial lesions, they were well reported in studies like Devkota et al., 12 Sharma et al.1 and Insler et al. 13
As noted by Loddenkemper et al. (2002), fiberoptic bronchoscopy remains the gold standard for diagnosing endobronchial lesion. 14 Low complication rates reported in this study further reinforces the safety of fiberoptic bronchoscopy. Complications such as bleeding, infection, and pneumothorax were minimal, as observed in similar studies. Diagnostic yield is typically high 3, 15 and bronchoscopy remains less invasive than CT-guided biopsies. In our study, 37.93% of the patients were previously started on empirical ATT elsewhere leading to delay in diagnosis. This emphasizes the need for early and accurate diagnostic tools like bronchoscopy. This finding echoes similar studies where the overlapping clinical presentation of tuberculosis and malignancies led to misdiagnosis. It is recommended that high-risk patients (e.g., those over 55 with significant smoking history) undergo bronchoscopy for malignancy before starting ATT.16 Clinicians should maintain a high index of suspicion for lung cancer in patients with tuberculosis, especially if they exhibit poor responses to treatment. 17 While bronchoscopy is effective, additional invasive procedures may be necessary for conclusive diagnoses, especially in cases with non-diagnostic results.18 In a cohort study, fiberoptic bronchoscopy yielded a malignancy diagnosis in 42% of cases, with endobronchial brushing proving more effective than Bronchoalveolar lavage. 19
Despite the strengths of bronchoscopy, it is essential to consider that its diagnostic yield can be limited in patients with prior anti-tubercular treatment, where symptoms may mimic malignancy.
Conclusion
Most lesions were malignant, majority of which, presented radiologically as mass, encountered most often in males, as risk factors like smoking are common in males. Most common endobronchial lesion was an exophytic lesion and commonly involving the right main bronchus. As squamous cell carcinoma is central in location and frequently associated with smoking, it was the most common (42.85%) histopathological variant, followed by adenocarcinoma (34.48%). In our study, 37.93% of the patients were previously started on empirical ATT elsewhere leading to delay in diagnosis, thereby highlighting the importance of bronchoscopy as an important tool in diagnosing malignancy. This study also reinforces the safety of flexible bronchoscopy as complications following the procedure were low, thereby avoiding the need for much invasive procedures like CT and Ultrasound guided biopsy