- Visibility 86 Views
- Downloads 12 Downloads
- DOI 10.18231/j.ijirm.2021.049
-
CrossMark

Effects of Sildenafil on spirometric pulmonary function parameters, pulmonary artery systolic pressure and BNP levels in patients with chronic obstructive pulmonary disease and erectile dysfunction
- Author Details:
-
 Keski Hakan *
Keski Hakan *
-
Demirtunç Refik
Introduction
Pulmonary hypertension (PH) is very prevalent among patients with chronic obstructive pulmonary disease (COPD). [1], [2] World Health Organization (WHO) classifies pulmonary hypertension associated with COPD as group 3 (pulmonary hypertension caused by lung diseases and/or hypoxia). [3] The presence of pulmonary hypertension is associated with increased mortality in this patient population. Apart from the treatment of the underlying disease and the nonspecific general measures such as loop diuretics and aldosterone antagonists, few choices are available for the treatment of PH in COPD population.
Erectile dysfunction (ED) is a common occurrence in patients with COPD. Unfortunately, many patients avoid the discussion of this issue with their health-care providers, which results in a decrease in their quality of life. Sildenafil, a phosphodiesterase 5 inhibitor, has a proven efficacy and safety profile in the treatment of ED in several patient populations. [4], [5], [6], [7], [8] Sildenafil has also been shown to be beneficial in patients with pulmonary arteriolar hypertension (group I). [9] However, there is no specific treatment recommended for the treatment of COPD-associated pulmonary hypertension (group 3) at present.
Despite the high frequency of ED as a comorbid condition in COPD patients, little data are available regarding the efficacy and safety of Sildenafil in COPD patients with ED. Instead, much effort has been concentrated on the evaluation of the effects of Sildenafil on pulmonary hypertension associated with COPD. Several studies, some of them randomized controlled, have shown the efficacy of Sildenafil in reducing pulmonary artery pressure in COPD patients irrespective of their status of ED. [10], [11] To the best of our knowledge, no study to date has evaluated the efficacy of Sildenafil in COPD patients who have both ED and PH.
Starting from their observation that two of their COPD patients who were treated with Sildenafil for ED reported subjective improvement in their dyspnea, Charan and colleagues, reported that Sildenafil improved forced expiratory volume in 1 second (FEV1) by 12% and 24% in these patients.[12] To our surprise, as far as we know, there are no data with respect to the effects of Sildenafil on the respiratory pulmonary function parameters in COPD patients. [12] Blanco et al., investigated the impact of Sildenafil on gas exchange in COPD patients with PH. The authors concluded that Sildenafil might impair arterial oxygenation at rest. [13] On the other hand, further observations have not confirmed the findings of this preliminary study. [14]
Brain type natriuretic peptide (NT-proBNP) is a well-recognized diagnostic and prognostic marker in patients with heart diseases, including left heart failure and myocardial infarction among others. [15] The acute exacerbations of COPD lead to increases in NT-proBNP blood levels, and this seem like an independent prognostic factor for mortality. [16], [17] More recently, Labaki and coworkers found that patients with stable COPD had higher NT-proBNP levels correlated with their GOLD stage, with the highest levels in GOLD stage D. [18] The authors showed that the higher the baseline serum level of NT-proBNP is, the more the future rate of acute exacerbations is. Moreover, NT-proBNP has been used as a successful tool for detecting the pulmonary hypertension in COPD patients. [19], [20] To our knowledge, only one study investigated the effect of Sildenafil on NT-proBNP levels in COPD patients with PH. The results of that study revealed that Sildenafil reduced both the PASP and the level of NT-proBNP significantly. [21]
Since pulmonary hypertension is common and associated with adverse clinical outcomes and increased mortality, the treatment of PH offers a feasible opportunity in reducing COPD related mortality. However, none of the studies to date has evaluated the effect of Sildenafil on pulmonary hypertension and spirometric pulmonary function parameters along with the levels of BNP in impotent COPD patients. Considering the high prevalence of ED among COPD patients, the question of how Sildenafil effects pulmonary function also demands answers. Hence, we aimed to evaluate the effects of Sildenafil on PASP as well as FEV1 and FVC and serum BNP levels in stable COPD patients with ED.
Materials and Methods
Study design, setting and patient selection
This was a prospective non-controlled interventional study that was conducted at the internal medicine clinic of the Haydarpaşa Numune Training Research Hospital in İstanbul, Turkey between December 2004 and May 2007. The local ethical committee granted approval of the study protocol. The study protocol was explained in detail to all participants, and written informed consent was signed by each participant.
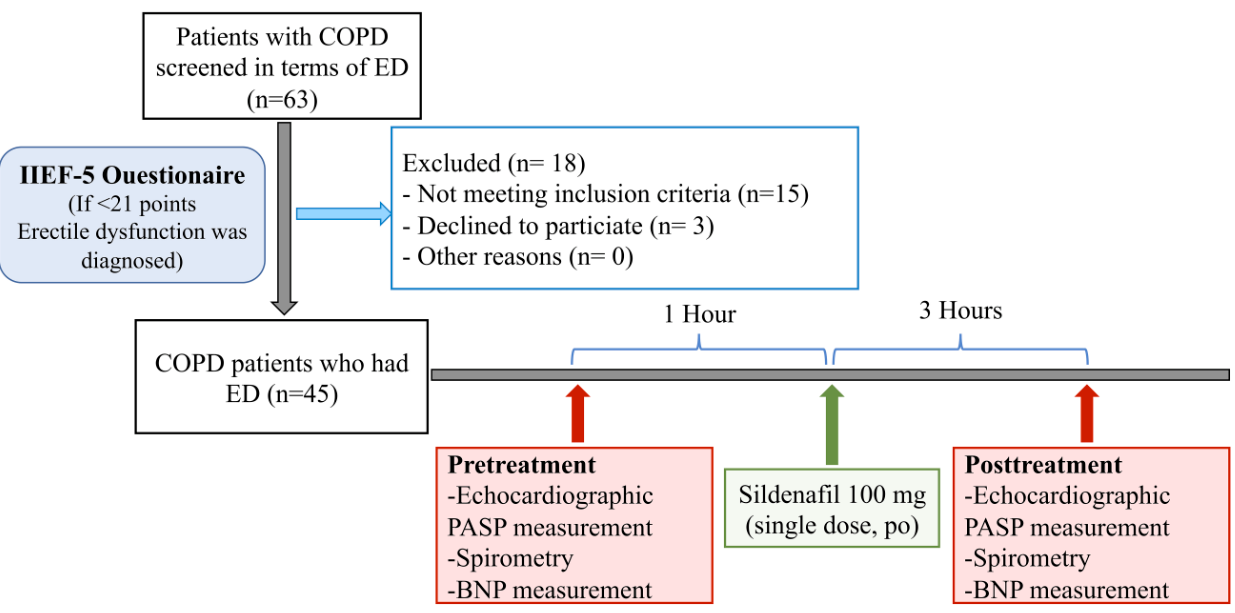
Consecutive patients with COPD who volunteered to complete the short form of International Index of Erectile Dysfunction Form (IIEF-5) were evaluated regarding the suitability for inclusion in the study. COPD patients, who were deemed to have erectile dysfunction based on IIEF-5 scores and systolic pulmonary artery pressure >45 mmHg (Stage 2 PH) based on echocardiographic measurement, were included in the study. Patients who had left heart failure, thoracic and/or diaphragm pathology, which might interfere with the echocardiographic and radiologic evaluations, were not involved in the study. In addition, patients with the following characteristics were excluded from the study: age <40 or >80 years, severe chronic liver disease, hypotension, severe valvular heart disease including aortic and mitral stenosis and/or insufficiency, and the use of nitrates. Patients who had dilated left atrium, a history of deep vein thrombosis and/or pulmonary embolism, pneumonia and/or COPD exacerbation, and coronary artery disease were kept out of the patient inclusion process. Coronary artery disease that required exclusion from the study was defined as having angina chest pain, pathologic Q waves and/or ischemic ST-T changes in electrocardiography or 50% or greater stenosis in coronary artery diameter with angiography. The patient selection process and the study design are depicted in [Figure 1].
Sildenafil administration and dose
Sildenafil (VİAGRA® Pfizer, Turkey) 100 mg was administered to each study participant orally once after the baseline spirometry, and the echocardiographic procedures and the blood draw for measurement of serum BNP levels. None of the patients experienced any adverse effects related to Sildenafil use. The same tests and measurements were performed 3 hours after the ingestion of Sildenafil when the effect of the drug was thought to be at its maximum level.
Data collection and tools
The diagnosis of COPD was made or had been made previously on the grounds of physical examination, chest X-ray, and spirometry findings in accordance with the GOLD criteria.[22]
Pulmonary hypertension
Pulmonary hypertension was assessed considering the clinical status of the patient as well as the findings of posteroanterior chest X-ray (increased cardiothoracic index, enlargement of hilar vascular structures, prominent pulmonary conus and upper lung vascular markings, >16 mm increase in the diameter of the right main descendent pulmonary artery) and ECG (P pulmonale, right axis deviation, right ventricular hypertrophy, and right ventricular overload). Echocardiographic measurements were performed with a Vivid 3 (General Electric, USA) machine by the same experienced cardiologist. A Doppler probe with 2.5 MHz was used for the evaluation. Transthoracic Doppler echocardiography performed while the patient was at rest. In the patients, in whom a tricuspid insufficiency was detected, the difference between the right ventricular peak pressure and the right atrial pressure was calculated. A 14-mmHg extra pressure value, which corresponded to the mean right atrial pressure, was added to this difference. The resultant pressure value was accepted as the pulmonary artery systolic pressure (PASP).
The patients were divided into three stages, based on their measured pulmonary artery pressure values: [23]
Stage I: Mild pulmonary hypertension (31-45 mmHg)
Stage II: Moderate pulmonary hypertension (46-70 mmHg)
Stage III: Severe pulmonary hypertension (>70 mmHg)
The patients with mild (stage I) pulmonary hypertension were excluded from the study.
Pulmonary function test (Spirometry)
Pulmonary function tests were performed 1 hour before the echocardiographic examination with a portable spirometer (Spirolab II, computerized pulmonary function laboratory). Three recordings were made for each patient. For the forced expiratory volume in 1 second (FEV1) and the forced vital capacity (FVC) values, the highest measured values, which derived from the three technically sufficient curves, were accepted as the final values. [24] For each patient, FVC, FEV1, the ratio of FEV1 to FVC (FEV1/FVC), and the maximum mid-expiratory flow rate (MMF, FEF25-75) values were recorded as the absolute values and the percent predicted. Korry Polpar’s reference value was used for the percent predicted. [25] The predicted values for each patient were determined as per sex, age, body weight and height; and the severity of the obstruction was graded based on the criteria of British Thoracic Society. [26] For each spirometry parameter, the measured values that were 79% or higher than the predicted ones, were accepted as normal, the values between 60-79% of the predicted as mild obstruction, the values between 40-59% as moderate obstruction and the values below 40% as severe airway obstruction.
Erectile dysfunction (ED)
Erectile dysfunction was assessed by self-administered IIEF-5 questionnaire. This questionnaire is the shortened form of the original International index of erectile function (IIEF) questionnaire, which was derived and validated by Rosen et al., [27] Turkish translation and validation study of the IIEF-5 was carried out by Turunc and colleagues. [28] IIEF-5 questionnaire is composed of 5 questions. Each question is scored between 0 and 5 points. If the sum of the points (IIEF-5 score) is below 21, it was accepted that the patient had erectile dysfunction.
Serum BNP measurements
The serum samples with EDTA were studied with chemiluminescent microparticle immunoassay in ARCHITECT iSystem (Abbott Laboratories) for BNP measurements.
Statistical analysis
Descriptive data derived from the study were presented as mean ± standard deviation and minimum and maximum if the continuous variables were normally distributed. Categorical variables were given as number and percentage in parenthesis. The normality check of continuous variables was performed by the Kolmogorov Smirnov test. Pre and post-treatment measurements of FEV1, FEV1/FVC, PASP and BNP were compared with the Paired t-test. The differences in each studied parameter were depicted as the box-plots. Statistical analysis was performed using SPSS for Windows (Version 16.0, SPSS Inc., Chicago, USA). Statistical significance level was accepted as p<0.05.
According to the power analysis that was based upon the pre- and post-treatment pulmonary hypertension measurements, the power of the study was calculated as 99% with 80% power and 5% type 1 error. Power analysis was performed with G*Power 3.1.9.4 for Windows package program.
Results
Overall, 45 male COPD patients between the ages of 49 and 79 were included in the study. The mean age of the study participants was 63.6 ± 8.3 years. The demographic characteristics and the baseline laboratory values and measurements of the study participants are shown in [Table 1].
Erectile dysfunction
The mean IIEF-5 score of the study population was 10.87 ± 3.33. None of the patients had been on drug treatment for ED. Overall, 19 patients had severe and 26 patients had moderate erectile dysfunction.
Spirometric measurements
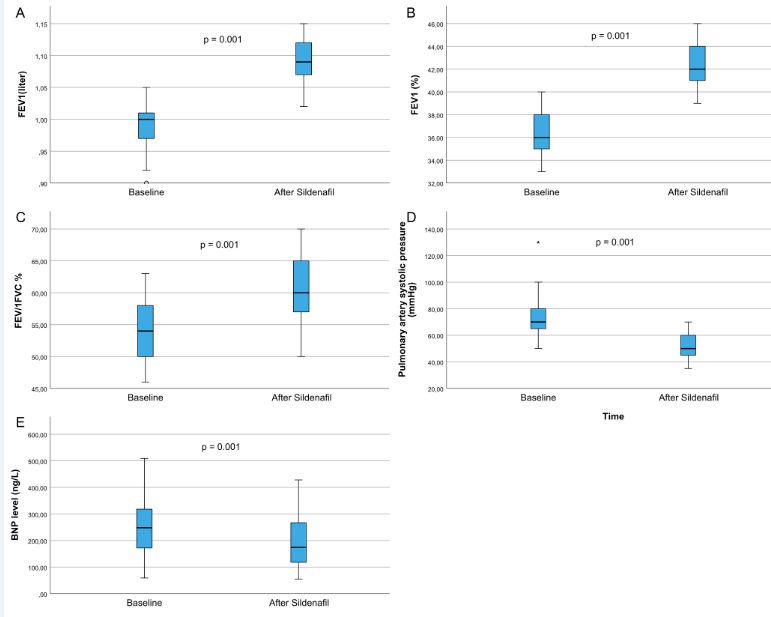
Both the percent predicted and the absolute FEV1 values significantly increased after the Sildenafil administration compared with the baseline values. The absolute amount of FEV1 increase was 0.09 L. Similarly, the FEV1/FVC ratio also increased significantly with the Sildenafil administration compared with the baseline values ([Table 2], [Figure 2] a, b).
Pulmonary artery pressures
Mean pulmonary artery systolic pressure decreased significantly from its baseline value with Sildenafil administration (Table 2, Figure 2c). The absolute amount of mean decrease in PASP was 12.58 ± 2.71 mmHg.
Serum brain type natriuretic peptide (BNP) values
The serum BNP values were significantly reduced with the Sildenafil administration compared with the pretreatment values (Table 2, Figure 2d).
|
|
Mean ± SD |
Min - Max. |
n (%) |
|
Age |
64.31 ± 8.24 |
49 - 79 |
|
|
Education |
|
|
|
|
Primary school |
|
|
20 (44) |
|
Secondary school |
|
|
16 (35.5) |
|
Illiterate |
|
|
9 (20) |
|
Comorbidities |
|
|
|
|
Hypertension |
|
|
11 (24.4) |
|
Coronary artery disease |
|
|
1 (2.2) |
|
Benign prostatic hyperplasia |
|
|
5 (11.1) |
|
Diabetes mellitus |
|
|
4 (8.9) |
|
Rheumatoid arthritis |
|
|
2 (4.4) |
|
IIEF-5 score |
10.87 ± 3.33 |
4 - 16 |
|
|
IIEF-5, Categorical |
|
|
|
|
0-10 |
|
|
19 (42.2) |
|
11-16 |
|
|
26 (57.8) |
|
FEV1 (L) |
0.99 ± 0.44 |
0.90 - 1.05 |
|
|
FEV1 (%) |
36.91 ± 15.33 |
33 - 40 |
|
|
FEV1/FVC |
55.11 ± 14.08 |
46 - 63 |
|
|
PASP (mmHg) |
69.78 ± 12.09 |
50 - 130 |
|
|
BNP (ng/L) |
243.96 ± 107.72 |
59 - 509 |
|
|
|
Baseline (Pretreatment) |
After Sildenafil administration |
p |
|
FEV1 (L) |
0.99 ± 0.44 |
1.08 ± 0.48 |
0.001 |
|
FEV1 (%) |
36.91 ± 15.33 |
40.60 ± 16.96 |
0.001 |
|
FEV1/FVC |
55.11 ± 14.08 |
59.79 ± 14.34 |
0.001 |
|
sPAP (mmHg) |
69.78 ± 12.09 |
57.20 ± 9.38 |
0.001 |
|
BNP level (ng/L) |
243.96 ± 107.72 |
185.80 ± 91.49 |
0.001 |
Discussion
The remarkable results of this present study were as follows: (i) Single 100 mg oral administration of Sildenafil reduced pulmonary artery systolic pressure significantly compared to the baseline values. (ii) The serum BNP levels significantly decreased by the Sildenafil administration compared with baseline levels. (iii) FEV1 and FEV1/FVC values showed a significant improvement with Sildenafil. This is the first study showing the pulmonary hemodynamic and spirometric beneficial effects of Sildenafil along with the serum BNP levels in COPD patients with erectile dysfunction.
Chronic obstructive pulmonary disease is considerably common in the general population. Thus, it ranked third among age-standardized death rates globally, following cardiovascular and cerebrovascular diseases. [29] PH frequently complicates the course of COPD. [30] The rate of the PH among COPD patients has been reported between 30% and 90%, depending on the study population and the various definitions and measurement tools of PH. [1], [2] Moreover, several studies have demonstrated that the presence and severity of PH are strongly correlated with the mortality rate in COPD patients. [2], [31] The exact pathophysiology of PH in COPD remains to be elucidated. However, chronic hypoxia is considered to play an important role in the development of PH. [32]
Erectile dysfunction is considered a harbinger of vascular disease. [33] ED is commonly encountered in patients with COPD. In a recent meta-analysis, Luo et al., reported that the risk of development of moderate to severe ED was approximately 2.5 times higher among COPD patients. [34] A number of epidemiologic studies reported the prevalence of ED among COPD patients up to 88%. [35], [36] Several factors were proposed as underlying pathophysiological links between COPD and ED, including hormonal imbalances, chronic hypoxia, smoking, and respiratory symptoms, to mention just a few. [34] Unfortunately, ED is not systematically evaluated in COPD patients in everyday practice. This might result from both the unwillingness of patients and their physicians. Since ED is indeed very prevalent among COPD patients, at least some of these patients may use phosphodiesterase-5 inhibitor drugs. Most of the attention has been given to the role of the prototype phosphodiesterase-5 inhibitor Sildenafil on pulmonary arterial hypertension. In patients with COPD, to our knowledge, almost all studies have evaluated the effects of Sildenafil either on pulmonary hypertension or on exercise capacity and the quality of life. None of the available studies has investigated the Sildenafil-induced changes in these parameters in impotent COPD patients. From this perspective, ours is the first study in the literature. We have detected erectile dysfunction in COPD patients with the self-administered IIEF-5 questionnaire and included these patients in the present study.
A number of studies have investigated the effect of Sildenafil on pulmonary hypertension that complicated COPD. Shrestha and colleagues randomized COPD patients with PH to receive either Sildenafil or optimal medical treatment. The results of this study showed that, compared to the controls, the reduction in pulmonary arterial systolic pressure and the increase in 6-minute walk test were significantly greater with Sildenafil treatment. Interestingly, Sildenafil improved Modified Medical Council Grade; a scale used to grade the severity of dyspnea. [11] Again, Blanco and colleagues conducted a randomized dose-comparison trial where they revealed that Sildenafil could reduce pulmonary arterial pressure both at rest and during exercise in COPD patients with PH. [13] However, Sildenafil impaired arterial oxygenation at rest. Thus, the authors supposed that Sildenafil might have worsened gas exchange because of the inhibition of hypoxic vasoconstriction, and warned that a close monitoring of blood gases would be prudent. However, more recent studies have not reproduced the results of the latter study in this respect. Vitolo and colleagues demonstrated the beneficial effects of Sildenafil on carbon monoxide diffusion capacity and BODE index. [14] We did not evaluate oxygenation in our study. In agreement with the published literature on the subject, our study showed significant reductions in pulmonary arterial systolic pressure values with Sildenafil use.
Interestingly, some studies revealed that Sildenafil did not have beneficial effects in terms of exercise performance in patients who had COPD without pulmonary hypertension. [37], [38] Thus, it seems plausible to speculate that beneficial effects of Sildenafil in COPD are principally obtained through the alleviation of pulmonary hypertension. The lack of beneficial effects on exercise capacity might have been due to the untoward effects of Sildenafil on the spirometric pulmonary function parameters as well. Unfortunately, there is scarcity of data regarding the effects of Sildenafil on the pulmonary function tests. Charan first observed spirometric FEV1 improvements in two patients with COPD and PH.12 To the best of our knowledge, there is no study assessing the effect of Sildenafil on the spirometric parameters in COPD patients with PH. We performed spirometric pulmonary function tests at baseline and after 3 hours of Sildenafil use. Our results showed significant improvements in both FEV1 and FEV1/FVC values. One indirect contribution to our results has come from the study by Rafiei et al., [39] The authors found that Sildenafil facilitated the weaning of COPD patients from the ventilator through improvements in ventilator parameters. [39]
Natriuretic peptides are biological hormones that are released from the heart in response to increased wall stress. BNP and its derivative NT-proBNP are well-established markers of myocardial function and their measurements are recommended in the diagnosis and management of heart failure. [40] Natriuretic peptides increase in patients with COPD during both stable disease and exacerbations and serve as a prognostic marker as well. [16], [17], [18] A recent meta-analysis has revealed that elevated levels of NT-proBNP levels predict all-cause mortality in COPD patients during both a stable disease and exacerbations. Moreover, this prediction is independent of the presence of confounding factors such as hypertension, and heart failure history, which are causes of NT-proBNP elevation per se. [41] The increase of natriuretic peptides is generally attributed to the increased pulmonary pressure and the related right ventricular strain and the associated cardiovascular comorbid situations in patients with COPD, the most common of which is heart failure. Our results also revealed the increased levels of serum NT-proBNP in stable COPD patients.
As far as we know, there is only one trial that has investigated the effect of Sildenafil on the levels of NT-proBNP in COPD patients with PH. Sharif-Kashani and colleagues conducted a trial study in which COPD patients with PH and baseline serum NT-proBNP >100 pg/mL were randomized either to amlodipine or Sildenafil treatment groups for two weeks. [21] Both drugs reduced pulmonary artery pressure and serum NT-proBNP levels significantly. Our results are in line with the study of Sharif-Kashani et al., in that the serum BNP levels were significantly reduced with a single dose Sildenafil treatment. [21]
This present study has some limitations that are worthy of mentioning. First, we did not conduct a placebo-controlled study. The study was open-labelled. Second, we did not use the gold standard method in the measurement of the pulmonary arterial systolic pressure, which was right heart catheterization. On the other hand, echocardiographic PASP measurement is preferred in daily practice due to its invasive nature, not widespread availability and higher cost. Moreover, it has been shown that echocardiographic PASP measurement showed a good correlation with the catheter method. [42] Third, we only evaluated the effects of one dose Sildenafil. It would be preferable to study the drug longer to evaluate the longer-term effects on the same studied parameters. Fourth, it would be better if we could have assessed the change in the severity of dyspnea in the patients. Despite these shortcomings, in several aspects, this current study presents some novel data.
In conclusion, the single-dose Sildenafil administration significantly reduced echocardiography-measured PASP. The serum level of BNP showed a significant decrease compared to the baseline. For the first time in the literature, we also showed that spirometric pulmonary function tests, namely FEV1 and FEV1/FVC ratio, significantly improved with the Sildenafil administration. This present study is the first study conducted in COPD patients who had PH as well as erectile dysfunction. Further long term studies are apparently needed to evaluate the efficacy of Sildenafil on erectile dysfunction and to assess its effects on pulmonary function tests, dyspnea, and respiratory system.
Acknowledgements
None.
Conflict of Interest
The author declares no potential conflicts of interest with respect to research, authorship, and/or publication of this article
Source of Funding
None.
References
- K Chatterjee, A R Tarawneh, S Alam. Out of proportion pulmonary hypertension in obstructive lung diseases. Curr Opin Pulm Med 2018. [Google Scholar] [Crossref]
- W Seeger, Y Adir, J A Barberà, H Champion, J G Coghlan, V Cottin. Pulmonary hypertension in chronic lung diseases. J Am Coll Cardiol 2013. [Google Scholar] [Crossref]
- R J Oudiz. Classification of Pulmonary Hypertension. Cardiol Clin 2016. [Google Scholar] [Crossref]
- N Ioakeimidis, J B Kostis. Pharmacologic therapy for erectile dysfunction and its interaction with the cardiovascular system. J Cardiovasc Pharmacol Ther 2014. [Google Scholar] [Crossref]
- P Shah, N Trivedi. A meta-analysis on efficacy and tolerability of Sildenafil for erectile dysfunction in patients with diabetes mellitus. Indian J Sex Transm Dis AIDS 2018. [Google Scholar] [Crossref]
- S Turk, Y Solak, S Kan, H Atalay, M Kilinc, E Agca. Effects of Sildenafil and vardenafil on erectile dysfunction and healthrelated quality of life in haemodialysis patients: A prospective randomized crossover study. Nephrol Dial Transplant 2010. [Google Scholar] [Crossref]
- C C Carson, A L Burnett, L A Levine, A Nehra. The efficacy of Sildenafil citrate (Viagra®) in clinical populations: an update. Urology 2002. [Google Scholar] [Crossref]
- G Mancia, T G Pickering, D B Glasser, J Orazem. Efficacy of Viagra® (Sildenafil citrate) in men with erectile dysfunction and arterial hypertension who are taking multiple antihypertensive treatments. 2002. [Google Scholar]
- S Bhogal, O Khraisha, M Al Madani, J Treece, S J Baumrucker, T K Paul, . Sildenafil for Pulmonary Arterial Hypertension. Am J Ther 2019. [Google Scholar] [Crossref]
- I Blanco, S Santos, J Gea, R Güell, F Torres, E Gimeno-Santos. Sildenafil to improve respiratory rehabilitation outcomes in COPD: A controlled trial. Eur Respir J 2013. [Google Scholar] [Crossref]
- S K Shrestha, B Srivastava, M Karki, D B Khatri, R M Pradhan. Effect of Sildenafil citrate on pulmonary arterial systolic pressure and sub-maximal exercise capacity in chronic obstructive pulmonary disease. Kathmandu Univ Med J 2017. [Google Scholar]
- N B Charan. Does Sildenafil also improve breathing?. Chest 2001. [Google Scholar] [Crossref]
- I Blanco, E Gimeno, P A Munoz. Hemodynamic and gas exchange effects of Sildenafil in patients with chronic obstructive pulmonary disease and pulmonary hypertension. Am J Respir Crit Care Med 2010. [Google Scholar] [Crossref]
- P Vitulo, A Stanziola, M Confalonieri, D Libertucci, T Oggionni, P Rottoli. Sildenafil in severe pulmonary hypertension associated with chronic obstructive pulmonary disease: A randomized controlled multicenter clinical trial. J Hear Lung Transplant 2017. [Google Scholar] [Crossref]
- J L Januzzi, C A Camargo, S Anwaruddin, A L Baggish, A A Chen, D G Krauser. The N-terminal Pro-BNP investigation of dyspnea in the emergency department (PRIDE) study. Am J Cardiol 2005. [Google Scholar] [Crossref]
- H Li, Z Zeng, J Cheng, G Hu, Y Li, L Wei. Prognostic Role of NT-proBNP for in-Hospital and 1-Year Mortality in Patients with Acute Exacerbations of COPD. Int J Chron Obstruct Pulmon Dis 2020. [Google Scholar] [Crossref]
- E Shafuddin, C L Chang, M Cooray, C M Tuffery, S J Hopping, G D Sullivan. Changes in biomarkers of cardiac dysfunction during exacerbations of chronic obstructive pulmonary disease. Respir Med 2018. [Google Scholar] [Crossref]
- W W Labaki, M Xia, S Murray, J L Curtis, R G Barr, S P Bhatt. NT-proBNP in stable COPD and future exacerbation risk: Analysis of the SPIROMICS cohort. Respir Med 2018. [Google Scholar] [Crossref]
- J Nowak, B Hudzik, J Niedziela, P Rozentryt, M Zembala, M Gąsior. Role of Pro-Brain Natriuretic Peptide Serum Concentration in the Detection of Pulmonary Hypertension in Patients With End-Stage Lung Diseases Referred for Lung Transplantation. Transplant Proc 2018. [Google Scholar] [Crossref]
- C U Andersen, S Mellemkjær, J E Nielsen-Kudsk, L D Sønderskov, B E Laursen, U Simonsen. Echocardiographic Screening for Pulmonary Hypertension in Stable COPD Out-Patients and NT-proBNP as a Rule-Out Test. COPD J Chronic Obstr Pulm Dis 2012. [Google Scholar] [Crossref]
- B Sharif-Kashani, A Hamraghani, J Salamzadeh, M Abbasi Nazari, M Malekmohammad, N Behzadnia, . The Effect of Amlodipine and Sildenafil on the NT-ProBNP Level of Patients with COPD-Induced Pulmonary Hypertension. Iran J Pharm Res IJPR 2014. [Google Scholar]
- D Singh, A Agusti, A Anzueto, P J Barnes, J Bourbeau, B R Celli. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease: the GOLD science committee report 2019. Eur Respir J 2019. [Google Scholar] [Crossref]
- G Simonneau, N Galiè, L J Rubin, D Langleben, W Seeger, G Domenighetti. Clinical classification of pulmonary hypertension. J Am Coll Cardiol 2004. [Google Scholar] [Crossref]
- F G Hoppin, N Cherniack. Pulmonary function tests for diagnosis and evaluation of COPD. Choronic Obstructive Pulmonary Disease 1991. [Google Scholar]
- M C Gerson. Cardiac Nuclear Medicine. 1987. [Google Scholar]
- . BTS Guidelines for the Management of Chronic Obstructive Pulmonary Disease. Thorax 1997. [Google Scholar] [Crossref]
- R Rosen, J Cappelleri, M Smith, J Lipsky, B Peña. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res 1999. [Google Scholar] [Crossref]
- T Turunç, S Deveci, S Güvel, L Peşkircioğlu. The assessment of Turkish validation with 5 question version of International Index of Erectile Function (IIEF-5). Turk J Urol 2007. [Google Scholar]
- K F Rabe, H Watz. Chronic obstructive pulmonary disease. Lancet 2017. [Google Scholar] [Crossref]
- I Singh, K C Ma, D A Berlin. Pathophysiology of Pulmonary Hypertension in Chronic Parenchymal Lung Disease. Am J Med 2016. [Google Scholar] [Crossref]
- K H Andersen, M Iversen, J Kjaergaard, J Mortensen, J E Nielsen-Kudsk, E Bendstrup. Prevalence, predictors, and survival in pulmonary hypertension related to end-stage chronic obstructive pulmonary disease. J Hear Lung Transplant 2012. [Google Scholar] [Crossref]
- A Chaouat, R Naeije, E Weitzenblum. Pulmonary hypertension in COPD. Eur Respir J 2008. [Google Scholar] [Crossref]
- J J Rodriguez, Al Dashti, R Schwarz, E R. Linking erectile dysfunction and coronary artery disease. Int J Impot Res 2005. [Google Scholar] [Crossref]
- L Luo, S Zhao, J Wang, Y Liu, Z Zhu, Q Xiang. Association between chronic obstructive pulmonary disease and risk of erectile dysfunction: a systematic review and meta-analysis. Int J Impot Res 2020. [Google Scholar] [Crossref]
- T-C Shen, W-C Chen, C-L Lin, C-H Chen, C-Y Tu, T-C Hsia. The Risk of Erectile Dysfunction in Chronic Obstructive Pulmonary Disease. Med (Baltimore) 2015. [Google Scholar] [Crossref]
- H Kahraman, B Sen, N Koksal, M Kilinç, S Resim. Erectile dysfunction and sex hormone changes in chronic obstructive pulmonary disease patients. Multidiscip Respir Med 2013. [Google Scholar] [Crossref]
- D J Lederer, M N Bartels, N W Schluger, F Brogan, P Jellen, B M Thomashow. Sildenafil for Chronic Obstructive Pulmonary Disease: A Randomized Crossover Trial. COPD J Chronic Obstr Pulm Dis 2012. [Google Scholar] [Crossref]
- S Holverda, H Rietema, H J Bogaard, N Westerhof, P E Postmus, A Boonstra. Acute effects of sildenafil on exercise pulmonary hemodynamics and capacity in patients with COPD. Pulm Pharmacol Ther 2008. [Google Scholar] [Crossref]
- M Rafiei, O Aghadavoudi, M Hojjat. The Effect of Sildenafil on Respiratory Weaning of Patients with Chronic Obstructive Pulmonary Diseases Admitted to Intensive Care Unit. Med Arch 2012. [Google Scholar] [Crossref]
- Jj V Mcmurray, S Adamopoulos, S D Anker, A Auricchio, M Bohm, K Dickstein. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart. Eur Heart J 2012. [Google Scholar] [Crossref]
- R Pavasini, G Tavazzi, S Biscaglia, F Guerra, A Pecoraro, F Zaraket. Amino terminal pro brain natriuretic peptide predicts all-cause mortality in patients with chronic obstructive pulmonary disease: Systematic review and meta-analysis. Chron Respir Dis 2017. [Google Scholar] [Crossref]
- H Gupta, G Ghimire, R Naeije. The value of tools to assess pulmonary arterial hypertension. Eur Respir Rev 2011. [Google Scholar] [Crossref]
- Introduction
- Materials and Methods
- Study design, setting and patient selection
- Sildenafil administration and dose
- Data collection and tools
- Pulmonary hypertension
- Pulmonary function test (Spirometry)
- Erectile dysfunction (ED)
- Serum BNP measurements
- Statistical analysis
- Results
- Erectile dysfunction
- Spirometric measurements
- Pulmonary artery pressures
- Serum brain type natriuretic peptide (BNP) values
- Discussion
- Acknowledgements
- Conflict of Interest
- Source of Funding