- Visibility 151 Views
- Downloads 20 Downloads
- Permissions
- DOI 10.18231/j.ijirm.2019.047
-
CrossMark

Clinicopathological profile of primary lung cancer in a tertiary care teaching hospital in the south-east coast of India
Abstract
Introduction: Lung is one of the commonest sites for neoplasms both primary and metastatic cancers. Identification and determination of histopathological play a major role in the diagnosis and treatment of cancer. Radiology and imaging helps in the selection of procedures to obtain a tissue sample for the diagnosis and management of lung cancer. The present study was aimed to analyze the clinic-pathological profile of primary lung cancer in the south-east coast of India.
Materials and Methods: A prospective, observational study was conducted in the Department of Pulmonary Medicine, Maharaja Institute of Medical Sciences (MIMS), Vizianagaram, Andhra Pradesh, India. A total of 104 patients with primary lung cancer were enrolled. Radiological, clinico pathological profile and Histopathological analysis was done individually for all patients.
Results: Male patients (70.1%) were more compared to females (29.9%). The Average age of the study population was 57.8 years. A total of 70(67.3%) study subjects had a history of smoking comprising of 61 males and 9 female subjects. Almost all study patients had clinical presentations of cough and shortness of breath (100%). Most common X-ray and CT chest radiographic feature was mass lesion (n=89 and n=91). Adenocarcinoma was identified in 79 patients (76.0%) as the most common histological type and it was also common in both smokers (n=49) and nonsmokers (n=29).
Conclusions: The most common histological variant was Adenocarcinoma followed by squamous cell carcinoma. Among men, smoking is the principal risk factor in the causation of lung cancer. A precise, accurate and rapid screening method is still warranted for the diagnosis of primary lung cancer.
Introduction
Lung cancer is one of the major oncological problems and incidence is increasing day by day due to smoking, environmental pollutants, and lung diseases. Morbidity and mortality due to lung cancer is growing gradually in developed and developing countries like India. Lung cancers are more common in men which had prevalence rate of new cases 11.3% and have a m ortality rate of 13.7% in India.[1],[2] In developed countries, lung cancer incidence is declined in men and constant plateau for females. In contrast to developed countries, incidence continues to rise for both males and females in India.[3]
The incidence of Small cell carcinoma is lesser compared to NSCLC but shows distinct clinical and pathological features. Radiological imaging plays a major and integral part in diagnosis, management, staging and follow up of lung cancer patients. Computed tomography (CT) scan helps in more accurate localization and anatomical details. It also gives vital clues towards histological diagnosis of malignancy like peripheral tumors as adenocarcinoma and central tumors as squamous cell carcinoma.
Early diagnosis of lung cancer may decrease cancer related mortality and increase the prognosis.[4] Cytology is a very good method for early evaluation, confirmation, and diagnosis of lung cancer. Moreover, it has fewer complications compared to other methods. Cytology with a combination of advanced radiographically guided sampling procedures is an important tool in the diagnosis of lung cancer.[5] The present study was conducted in a tertiary care teaching hospital to evaluate the clinico pathological profile of primary lung cancer.
Materials and Methods
A prospective, observational study was conducted in the Department of Pulmonary Medicine, Maharaja Institute of Medical Sciences (MIMS), Vizi anagaram, Andhra Pradesh, India. The study was carried out for a period of three years between March 2016 and March 2019. The study was approved by the scientific committee as well as the Institutional Ethics Committee. Informed consent was obtained from all of the study participants. The study was conducted according to the Declaration of Helsinki.
A total of 104 cases of primary lung cancer was diagnosed radiologically and histopathologically were enrolled for the study. The Clinico pathological profile of primary lung cancer patients was suspected and evaluated based on routine clinical investigations like X- ray, computed tomography of the chest, bronchoalveolar lavage (BAL), bronchoscopy was included. Bleeding disorders, uremia and tuberculosis positive sputum microscopy cases were excluded from the study. Above mentioned parameters could be important risk factors for spontaneous bleeding diathesis and bleeding in uremia which can complicate the procedure of Fine-needle aspiration cytology (FNAC)/ transbronchial needle aspiration (TBNA) and biopsy. Only patients with sputum negative with radiological opacities were selected for FNAC or TBNA, whereas antituberculosis treatment under RNTCP was started immediately for sputum microscopy positive cases and patients were followed up.
Results
A total of 104 patients with primary lung cancer were included in the present study. Male patients (70.1%) were more compared to females (29.9%). Nearly 80.0% of the study subjects were between the age group of 40-60 years. The Average age of the study population was 57.8 years. Baseline characteristics and age distribution of study participants were showed in [Table 1] .
| Characteristic | Number (n=104) |
| Gender, n (%) | |
| Male | 73 (70.1) |
| Female | 31 (29.9) |
| Age in years (Mean±SD) | 57.85±11.23 |
| Age group, frequency (%) | |
| 20-30 | 03 (2.0%) |
| 31-40 | 03 (2.0%) |
| 41-50 | 27 (25.9%) |
| 51-60 | 29 (27.8%) |
| 61-70 | 30 (28.8%) |
| >71 | 12 (11.5%) |
| Smoking status, n (%) | |
| Smokers | 70 (67.3%) |
| Non-smokers | 34 (32.7%) |
A total of 70 (67.3%) study subjects had a history of smoking comprising of 61 males and 9 female subjects. Distribution of smokers and Nonsmokers among study subjects were showed in [Table 1].
Most of the patients had multiple presenting complaints. Almost all study patients had clinical presentations of cough and shortness of breath (100%). A total of 29 patients had cough with expectoration. The second most common presentation was loss of appetite (56.7%) followed by hemoptysis (28.8%), wheezing (10.5%) respectively. The Frequency of individual symptoms among study subjects with primary lung cancer were showed in [Table 2].
| Symptom | Number of patients (N=104) | Percentage (%) |
| Cough | 104 | 100 |
| Shortness of breath | 104 | 100 |
| Loss of Appetite | 59 | 56.7 |
| Hemoptysis | 30 | 28.8 |
| Expectoration | 29 | 27.8 |
| Wheezing | 11 | 10.5 |
| Chest pain | 9 | 8.6 |
| Fever | 0 | 0 |
X-ray chest
Radiologically, most of the patients in our study had multiple findings. The most common chest radiographic feature was mass lesion (n=89). Mass with lung collapse was found in 3 patients, while mass with pleural effusion was identified in 28 patients. The other radiological appearances were the collapse of the left lung in 7 patients, pleural effusion in 34 patients and consolidation in 9 patients. Bilateral lower lobe opacities, metastasis, and obstructive pneumonia were observed in 3, 2 and 1 respectively. The Frequency of individual findings on chest X-ray among study subjects were listed in [Table 3].
CT-Thorax
CT thorax was done in all study patients. The most common CT feature was mass lesion which was detected in 91 patients (87.5%). Bilateral multiple nodules were seen in 1 (0.9%). Bronchus compression and metastasis were found in 5 (4.8%) cases each. The Frequency of individual findings on CT Thorax among study subjects was showed in [Table 3].
| Finding | Chest X-ray, n (%) | CT Thorax, n (%) |
| Lung mass | 89(85.5) | 91(87.5) |
| Collapse of lung | 11(10.5) | 11(10.5) |
| Pleural effusion | 34(32.6) | 33(31.7) |
| Lung Consolidation | 9(8.6) | 1(0.9) |
| Lung cavity | 5(4.8) | 2(1.8) |
| Obstructive pneumonia | 1(0.9) | 3(2.8) |
| Bilateral multiple nodules | 1(0.9) | 1(0.9) |
| Bilateral lower lobe opacities | 3(2.8) | 4(3.8) |
| Bronchus compression | - | 5(4.8) |
| Metastasis | 2(1.8) | 5(4.8) |
A total of 50 (48.0%) study subjects had narrowed bronchus and 42 subjects showed normal airways after bronchoscopy. Other than narrowing, few subjects showed endobronchial mass (n=10), extrinsic compression (n=1) and erythematous patch (n=1) respectively. The Frequency of individual bronchoscopy findings among study subjects were listed in [Table 4].
| Finding | Number | Percentage |
| Normal | 42 | 40.3 |
| Bronchus narrowed | 50 | 48.0 |
| Endobronchial mass | 10 | 9.6 |
| Extrinsic compression | 1 | 0.9 |
| Erythematous patch | 1 | 0.9 |
Adenocarcinoma was identified in 79 patients (76.0%) as the most common histological type of lung cancer in the present study. Out of 79 patients, 51(64.5%) patients were males and 28(35.5%) were female patients. The second common type was squamous cell carcinoma which was seen in 18 patients (17.3%). There were 5 cases of small cell carcinoma and 2 cases of mesothelioma were observed in the study. Bronchoalveolar lavage (BAL) fluid cytology had showed normal in 65 patients and adenocarcinoma in 31 study subjects and 8 cases with squamous cell carcinoma. Histopathological profile of study subjects with primary l ung cancer was showed in [Table 5].
| Histopathological Type | Number | Percentage |
| FNAC/TBNA cytology | ||
| Adenocarcinoma | 79 | 76.0 |
| Squamous cell carcinoma | 18 | 17.3 |
| Small cell carcinoma | 5 | 4.8 |
| Mesothelioma | 2 | 1.9 |
| Bronchoalveolar lavage (BAL) fluid cytology | ||
| Normal | 65 | 62.5 |
| Adenocarcinoma | 31 | 29.8 |
| Squamous cell carcinoma | 8 | 7.6 |
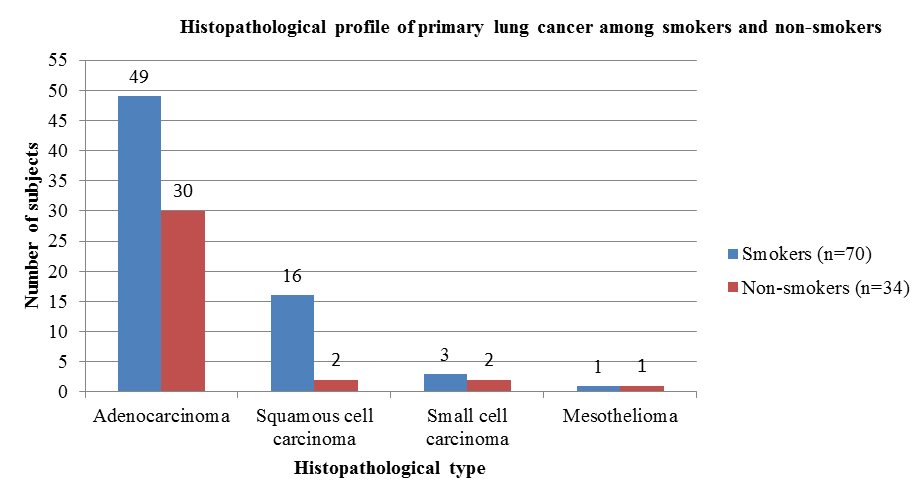
Adenocarcinoma was the most common histopathological type observed in both smokers (n=49) and nonsmokers (n=29). Squamous cell carcinoma was the second most type observed in 16 smokers and 2 non-smokers. Small cell carcinoma and mesothelioma were observed in 3 and 1 smokers and 2 and 1 non-smokers respectively. Histopathological profile of study subjects among smokers and non-smokers were showed in [Figure 1].
Discussion
In the present study, the mean age of lung cancer was 57.8 years which is a known fact that lung cancer is a disease of old age. This finding is consistent with studies conducted by Kumar et al., in North India and Dhandapani et al., in South India, both of which showed a mean age group close to 60 years.[6],[7] However, our study reported a wide range of age group s from 20 to 85 years. Sharma DK et al conducted a study and showed a similar range of age groups.[6] The male to female ratio in the present study was 2.35:1 which indicates that lung cancer incidence is showing an increasing trend among females. Similarly, the smoker to non-smoker ratio of lung cancer in the present study was 2.05:1 which clearly implies that lung cancer is showing a rising trend again among the non-smoker population. Our study findings were consistent with other published articles.[8],[9]
The incidence and prevalence rates of respiratory system cancers are different in various parts of India. Several studies across India[10] including reports of the National Cancer Registry Program (NCRP)[11] had reported that laryngeal cancer was the most common site. The present study was in agreement with the previously published articles where the lung was the topmost site for malignancy in males both smokers and non-smokers.
In the present study, several weeks of cough and shortness of breath are the most common symptoms along with loss of appetite, hemoptysis, cough with expectoration wheezing and chest pain. This study is similar to a publishedin the literature from different part s of India. [3],[12],[13] Surprisingly, fever was not complained by anyone during the entire period of the study.
Most of the study subjects had multiple findings on chest X-ray. Lung mass (85.5%), pleural effusion (32.6%), collapse (10.5%), consolidation (8.6%) and these findings were like other studies.[6],[14] Compared to other histological variants, squamous cell cancer h as few variations in radiology. Cavitation was unique to squamous type and not seen in adenocarcinoma. Some studies reported cavitation in adenocarcinoma patients which was not seen in the present study.[14]
Compare to the other studies, the present study has shown higher radiological variations in chest CT which includes bronchus compression (4.8%), bilateral lower lobe opacities (3.8%), obstructive pneumonia (2.8%), bilateral multiple nodules (0.9%). A study conducted by Gupta et al., and reported that more incidence of mediastinal adenopathy (79% vs 31%). [14] Another study conducted by Govindaraj et al., and concluded that metastasis to contralateral lung was higher in the study (20.6% vs 4.6%).[15] Two separate studies conducted by Kumar et al., and Gupta et al, also reported that consolidation was common in adenocarcinoma compared to other histological types. The Same studies also reported the clinical findings of clubbing and Pancoast syndrome were common in squamous cell carcinoma histology compared to others. [6],[14]
Bronchoscopy is one of the most useful and precise diagnostic procedure in the evaluation of the suspected cases of endobronchial lung cancer. In the al peripheral tumors, Radial probe endobronchial ultrasound (EBUS) helps in the evaluation and sampling. CT guided FNAB is procedure was done in our study which as very high complications as seen in previous Indian [16],[17] and International studies[18],[19] published earlier. In the present study, the overall yield wit h bronchoscopy was 58.67% and FNAB was 53.24%.
Broncho-alveolar lavage (BAL) is the saline lavage that explores large areas of the alveolar compartment obtaining cellular as well as non-cellular constituents of the lower respiratory tract. BAL is a good diagnostic tool for the diagnosis of pulmonary malignancy conditions like bronchoalveolar cell carcinoma.
Adenocarcinoma (76.0%) was the most common type of cancer in males and females as well as smokers and non-smokers. This higher incidence may be due to non-active smoking exposures like second - hand smoke exposure, air pollution, and genetic factors. Squamous cell carcinoma contributes 17.3% of the study population which comprises 15.3% of smokers. Squamous cell carcinoma showed a causal relationship with smoking history and higher incidence was seen in males compared to females. This is in concordance with several studies. [6],[7],[14],[20] The incidence and pattern of primary lung cancer have been changing continuously over the last decade in India as well as in western countries. Several published reports stated that lung cancer is being increasingly diagnosed in women[21] as compared to males and adenocarcinoma is slowly overtaking small cell carcinoma[15] but some studies were inconsistent with our findings.[12],[22],[23]
Cough is the most common presenting symptom in adenocarcinoma and squamous cell carcinoma histology, whereas hemoptysis was more common in squamous cell carcinoma. Out of 79 adenocarcinoma cases, 12 patients had consolidation like clinical features on presentation. The limitations of the present study were followed up and the survival of patients could not be done in the study participants. Stage identification and distribution were not performed and treatment modalities with response rates were not assessed.
Conclusions
Although lung cancer is the disease of old age, it may occur even at a young age also. In the present study, one study participant had twenty years of age. Primary lung cancer incidence and mortality are slowly increasing in non-smokers also. The most common histological variant was Adenocarcinoma followed by squamous cell carcinoma. Among men, smoking is the principal risk factor in the causation of lung cancer in the present study. Individuals who have long experience of unexplained cough with other symptoms like weight loss, shortness of breath with non-resolving collapse-consolidation on chest radiographs are the primary signs and diagnostic findings for the identification of primary lung cancer.
Source of funding
None.
Conflict of interest
None.
Acknowledgement
None.
References
- . Lung Cancer in India: Challenges and Perspectives. J Thorac Oncol. 2017;12(1):114-115. [Google Scholar]
- Noronha V, Pinninti R, Patil VM, Joshi A, Prabhash K. Lung cancer in the Indian subcontinent. South Asian J Cancer. 2016;5(3):95-103. [Google Scholar]
- Behera D, Balamugesh T. Lung cancer in India. Indian J Chest Dis Allied Sci. 2004;46(4):269-281. [Google Scholar]
- Hirsch FR, Franklin WA, Gazdar AF, Bunn PA. Early Detection of Lung Cancer: Clinical Perspectives of Recent Advances in Biology and Radiology. Clin Cancer Res. 2001;7(1):5-22. [Google Scholar]
- Midthun DE. Early detection of lung cancer. F1000 Research . . 2016;5. [Google Scholar]
- Sharma DK, Kumar M, Garg M, Jain P. Clinicopathological Profile of Lung Cancer - Changing Trends in India. Int J Res Med. 2016;5:57-62. [Google Scholar]
- Dhandapani S, Srinivasan A, Rajagopalan R, Chellamuthu S, Rajkumar A, Palaniswamy P. Clinicopathological Profile of Lung Cancer Patients in a Teaching Hospital in South India. J Cardio-Thorac Med. 2016;4(2):440-443. [Google Scholar]
- Malik PS, . RV. Lung cancer: prevalent trends & emerging concepts. Indian J Med Res. 2015;141(1):5-7. [Google Scholar]
- Noronha V, Dikshit R, Raut N, Joshi A, Pramesh CS, George K. Epidemiology of lung cancer in India: Focus on the differences between non-smokers and smokers: A single-center experience. Indian J Cancer. 2012;49(1). [Google Scholar]
- Malhotra V, Shah BS, Sabharwal S. Pattern of cancer in Dayanand Medical College & Hospital, Ludhiana (a ten- year retrospective study). Indian J Pathol Microbiol. 2001;44(1):27-30. [Google Scholar]
- . NCRP Anual Reports. . 2019. [Google Scholar]
- Rawat J, Sindhwani G, Gaur D, Dua R, Saini S. Clinico-pathological profile of lung cancer in Uttarakhand. Lung India Organ Indian Chest Soc. 2009;26(3):74-76. [Google Scholar]
- Agrawal A, Tandon R, Singh L, Kumar P, Pant H, Prakash S. Clinical profile of lung cancer in a tertiary care teaching hospital in north India with special reference to acceptance and outcome of treatment. J Pulmonol. 2018;2(1):1-10. [Google Scholar]
- Gupta R, Chowdhary I, Singh P. Clinical, radiological and histological profile of primary lung carcinomas. JK Sci. 2015;17(3):146-146. [Google Scholar]
- Govindaraj V, Soman R, Saka V, Badhe B, Dubashi B. Clinico-pathological profile of primary lung cancer in a tertiary care center in South India. Indian J Immunol Respir Med. 2018;3(4):165-169. [Google Scholar]
- Dash BK, Tripathy SK. Comparison of accuracy and safety of computed tomography-guided and unguided transthoracic fine-needle aspiration biopsy in diagnosis of lung lesions. J Assoc Physicians India. 2001;49:626-629. [Google Scholar]
- Mohapatra PR, Saini V. Comparison of accuracy and safety of CT guided and unguided transthoracic FNAB in diagnosis of lung lesions. J Assoc Physicians India. 2003;51:88-88. [Google Scholar]
- Kaneko M, Eguchi K, Ohmatsu H, Kakinuma R, Naruke T, Suemasu K. Peripheral lung cancer: screening and detection with low-dose spiral CT versus radiography. Radiology. 1996;201(3):798-802. [Google Scholar]
- Larscheid RC, Thorpe PE, Scott WJ. Percutaneous transthoracic needle aspiration biopsy: a comprehensive review of its current role in the diagnosis and treatment of lung tumors. Chest. 1998;114(3):704-709. [Google Scholar]
- Malik PS, Sharma MC, Mohanti BK, Shukla NK, Deo S, Mohan A. Clinico-pathological profile of lung cancer at AIIMS: a changing paradigm in India. Asian Pac J Cancer Prev APJCP. 2013;14(1):489-494. [Google Scholar]
- Prasad R, Srivastava AN, Verma SK. Clinico-pathological Profile of Bronchogenic Carcinoma Among Females in North India. Indian J Chest Dis Allied Sci. 2015;57(3):161-163. [Google Scholar]
- Jindal S, Malik SK, Datta BN. Lung cancer in Northern India in relation to age, sex and smoking habits. Eur J Respir Dis. 1987;70(1):23-38. [Google Scholar]
- Baburao A, Narayanswamy H. Clinico-Pathological Profile and Haematological Abnormalities Associated with Lung Cancer in Bangalore, India. Asian Pac J Cancer Prev. 2016;16(18):8235-8238. [Google Scholar]